A new study of mitochondrial DNA in ME/CFS patients has provided some important clues as to the variation of symptoms seen in patients.
Four important points brought out
in this study were:
1) None of the patients showed any evidence of a mitochondrial genetic disease.
2) No difference was seen in the types of mitochondrial DNA between patients and healthy individuals
3) There was no increased susceptibility to ME/CFS among people with different mitochondrial SNPs (single variations in DNA)
4) However, there were associations of SNPs with certain symptoms and/or their severity. Individuals that carry a particular SNP, for example, are predicted to be at greater risk of experiencing particular types of symptoms once they become ill. (Single nucleotide polymorphisms, frequently called SNPs (pronounced “snips”), are the most common type of genetic variation among people.)
What this means is that 1) ME/CFS is not genetic, 2) ME/CFS patients do not have pre-dispositions for getting the disease, and 3) there may be a single pathogen causing the disease.
The authors conclude:
"A puzzling aspect of ME/CFS has been the diversity of symptoms and the variation of their severity among different individuals. These differences should not be taken as proof that more than one insult was the initiating factor, nor that different patients have different underlying problems. It remains possible that much of the diversity of the manifestation of the illness results from genetic diversity rather than the existence of multiple fundamental causes."
This study provides a rationale for outbreaks and clusters. It also accounts for both the discrepancies in Fukuda, CCC, and ICC clinical case definitions as well as the large number of possible combinations of symptoms. These case definitions may be describing the same illness, caused by the same pathogen, as it is experienced by people with distinct genetic variations.
The findings of this study represent a major shift in thinking, not just about ME/CFS, but about all diseases. This study explains how a single pathogen can create multiple symptoms, and how those symptoms may manifest themselves depending on genetic variations in the host. The findings also may account for ranges in severity.
You can read about the Chronic Fatigue Initiative HERE.
______________________________________
Mitochondrial DNA and ME/CFS : A Guide to the Hanson Lab's 2016 JTM Publication
By Maureen Hanson
This is a simplified explanation of the 2016 academic paper published in the Journal of Translational Medicine.
Mitochondrial DNA variants correlate with symptoms in myalgic encephalomyelitis/chronic fatigue syndrome by Paul Billing-Ross, Arnaud Germain, Kaixiong Ye, Alon Keinan, Zhenglong Gu, and Maureen R. Hanson. J. Translational Medicine. 2016, 14:19
Patients with ME/CFS experience a profound lack of energy, severe fatigue, along with a variety of other symptoms, including one or more of the following: muscle pain, headaches, gastrointestinal discomfort, difficulty concentrating, exacerbation of symptoms following exercise, abnormal regulation of blood pressure and heart rate, and unrefreshing sleep. Mitochondria, sub-cellular organelles are responsible for producing ATP, the energy coinage of the cell, through conversion of glucose. Therefore, a logical approach to learn more about a disease affecting energy is probing of the function of mitochondria.
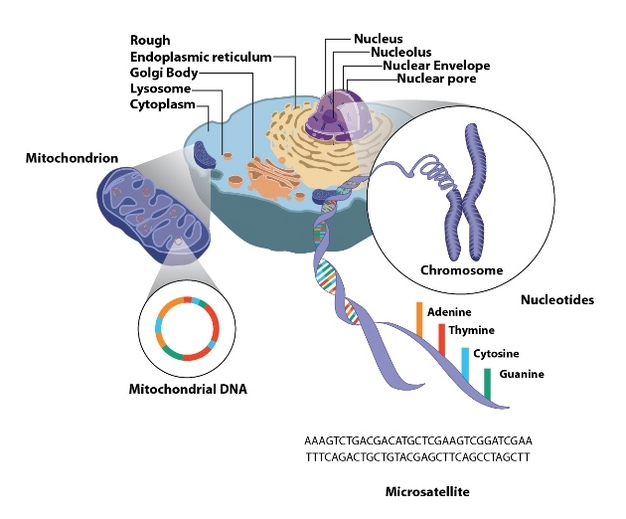
Mitochondria are made up of molecules encoded by the nuclear genome--DNA located in the nucleus--as well as the mitochondrial genome—a small amount of DNA present within each organelle. Defects in mitochondrial DNA lead to devastating genetic diseases, with such symptoms as brain abnormalities, severe fatigue, blindness or defective heart function—and can be fatal. The mitochondrial genome of healthy humans also exhibits some natural variation—a single component of the mitochondrial DNA sometimes differs between one human and another—this is known as a SNP (single nucleotide polymorphism, "snip"). Often more than one SNP differs between one population of humans and another—for example, mitochondrial genomes whose origin can be traced to France differ in a number of SNPs from those in people in Central Asia. These different types of mitochondrial genomes, based on a specific set of SNPs, are referred to as haplogroups. Even people whose mitochondrial DNA belongs to the same haplogroup can differ among one another because of some variation in additional SNPs. Some mitochondrial SNPs have been associated with various characteristics, such as adaptation to cold weather or high altitude environments and have been implicated in susceptibility to diabetes and various inflammatory diseases. Aninformative review of the role of mitochondria in disease has been written by Wallace and Chalkia, researchers at the University of Pennsylvania.
A further complexity of mitochondrial genetics is that there are many individual mitochondria within the same cell, and thus many copies of mitochondrial DNA in each cell. Sometimes new mutations arise so that some of the copies of DNA within the same cell, and therefore within the same person, differ from one another. This situation is called “heteroplasmy”. As cells grow and multiply, by chance there can be uneven distribution of normal vs. abnormal DNA to different cells. If mitochondrial DNA with a harmful mutation becomes the predominant type in a particular tissue, serious symptoms will emerge.
In our JTM paper, work that was primarily supported by the Chronic Fatigue Initiative, we sequenced the mitochondrial DNA from a cohort of ME/CFS patients and healthy individuals, using DNA extracted from white blood cells stored in the biobank developed by the Chronic Fatigue Initiative.
We asked four primary questions:
Furthermore, we found no difference in the degree of heteroplasmy between patients and healthy individuals.
We also observed no increased susceptibility to ME/CFS among individuals carrying particular haplogroups or SNPs within a haplogroup.
However, we did detect associations of particular SNPs with certain symptoms and/or their severity. For example, we did find that individuals with particular SNPs were more likely to have gastrointestinal distress, chemical or light sensitivity, disrupted sleep, or flu-like symptoms. This finding does NOT mean that if your mitochondrial DNA carries one of these SNPs, you will inevitably experience a particular symptom or have higher severity of some symptoms. Instead, because a particular SNP was seen more often in ME/CFS patients with certain characteristics, individuals that carry that SNP are predicted to be at greater risk of experiencing particular types of symptoms once they become ill.
This study demonstrates the importance of a well-characterized cohort of patients and controls along with detailed clinical information about their experience of illness. Without the data from the lengthy patient questionnaires collected along with the subject’s blood, we could not have correlated SNPs with patient characteristics. While the materials from the CFI subjects are extremely valuable and our results are statistically significant, greater numbers of subjects must be analyzed to determine whether the correlations we detected continue to hold up when more patients are studied, and whether such correlations exist within people carrying other haplogroups.
Due to the European origin of most of the ancestors of the CFI subjects, most belong to haplogroup H, the most common European haplogroup. A much larger number of haplogroup H subjects, as well as large cohorts of individuals with other haplogroups, will be necessary to analyze to dissect out other possible correlations or to determine whether or not any of the correlations we detected with a relatively small population are spurious. With more subjects, we might also be able to detect additional correlations that were not obvious from our initial study.
Whether or not the genetic correlations we have observed are verified or not through further work, our study indicates an important hypothesis that should be tested in ME/CFS. How much of the variation in symptoms between different individuals results from their different nuclear and/or mitochondrial genetic makeup, rather than variation in the inciting cause?
A puzzling aspect of ME/CFS has been the diversity of symptoms and the variation of their severity among different individuals. These differences should not be taken as proof that more than one insult was the initiating factor, nor that different patients have different underlying problems. It remains possible that much of the diversity of the manifestation of the illness results from genetic diversity rather than the existence of multiple fundamental causes.
This article was written by Professor Maureen Hanson and is licensed under a Creative Commons Attribution 4.0 International License.
Maureen R. Hanson
Liberty Hyde Bailey Professor
[email protected]
Phone: 607-254-4833
Fax: 607-255-6249
Hanson Laboratory
Department of Molecular Biology and Genetics
321 Biotechnology Building
Cornell University
Ithaca, NY 14853
Phone: 607-254-4832
Four important points brought out
in this study were:
1) None of the patients showed any evidence of a mitochondrial genetic disease.
2) No difference was seen in the types of mitochondrial DNA between patients and healthy individuals
3) There was no increased susceptibility to ME/CFS among people with different mitochondrial SNPs (single variations in DNA)
4) However, there were associations of SNPs with certain symptoms and/or their severity. Individuals that carry a particular SNP, for example, are predicted to be at greater risk of experiencing particular types of symptoms once they become ill. (Single nucleotide polymorphisms, frequently called SNPs (pronounced “snips”), are the most common type of genetic variation among people.)
What this means is that 1) ME/CFS is not genetic, 2) ME/CFS patients do not have pre-dispositions for getting the disease, and 3) there may be a single pathogen causing the disease.
The authors conclude:
"A puzzling aspect of ME/CFS has been the diversity of symptoms and the variation of their severity among different individuals. These differences should not be taken as proof that more than one insult was the initiating factor, nor that different patients have different underlying problems. It remains possible that much of the diversity of the manifestation of the illness results from genetic diversity rather than the existence of multiple fundamental causes."
This study provides a rationale for outbreaks and clusters. It also accounts for both the discrepancies in Fukuda, CCC, and ICC clinical case definitions as well as the large number of possible combinations of symptoms. These case definitions may be describing the same illness, caused by the same pathogen, as it is experienced by people with distinct genetic variations.
The findings of this study represent a major shift in thinking, not just about ME/CFS, but about all diseases. This study explains how a single pathogen can create multiple symptoms, and how those symptoms may manifest themselves depending on genetic variations in the host. The findings also may account for ranges in severity.
You can read about the Chronic Fatigue Initiative HERE.
______________________________________
Mitochondrial DNA and ME/CFS : A Guide to the Hanson Lab's 2016 JTM Publication
By Maureen Hanson
This is a simplified explanation of the 2016 academic paper published in the Journal of Translational Medicine.
Mitochondrial DNA variants correlate with symptoms in myalgic encephalomyelitis/chronic fatigue syndrome by Paul Billing-Ross, Arnaud Germain, Kaixiong Ye, Alon Keinan, Zhenglong Gu, and Maureen R. Hanson. J. Translational Medicine. 2016, 14:19
Patients with ME/CFS experience a profound lack of energy, severe fatigue, along with a variety of other symptoms, including one or more of the following: muscle pain, headaches, gastrointestinal discomfort, difficulty concentrating, exacerbation of symptoms following exercise, abnormal regulation of blood pressure and heart rate, and unrefreshing sleep. Mitochondria, sub-cellular organelles are responsible for producing ATP, the energy coinage of the cell, through conversion of glucose. Therefore, a logical approach to learn more about a disease affecting energy is probing of the function of mitochondria.
Mitochondria are made up of molecules encoded by the nuclear genome--DNA located in the nucleus--as well as the mitochondrial genome—a small amount of DNA present within each organelle. Defects in mitochondrial DNA lead to devastating genetic diseases, with such symptoms as brain abnormalities, severe fatigue, blindness or defective heart function—and can be fatal. The mitochondrial genome of healthy humans also exhibits some natural variation—a single component of the mitochondrial DNA sometimes differs between one human and another—this is known as a SNP (single nucleotide polymorphism, "snip"). Often more than one SNP differs between one population of humans and another—for example, mitochondrial genomes whose origin can be traced to France differ in a number of SNPs from those in people in Central Asia. These different types of mitochondrial genomes, based on a specific set of SNPs, are referred to as haplogroups. Even people whose mitochondrial DNA belongs to the same haplogroup can differ among one another because of some variation in additional SNPs. Some mitochondrial SNPs have been associated with various characteristics, such as adaptation to cold weather or high altitude environments and have been implicated in susceptibility to diabetes and various inflammatory diseases. Aninformative review of the role of mitochondria in disease has been written by Wallace and Chalkia, researchers at the University of Pennsylvania.
A further complexity of mitochondrial genetics is that there are many individual mitochondria within the same cell, and thus many copies of mitochondrial DNA in each cell. Sometimes new mutations arise so that some of the copies of DNA within the same cell, and therefore within the same person, differ from one another. This situation is called “heteroplasmy”. As cells grow and multiply, by chance there can be uneven distribution of normal vs. abnormal DNA to different cells. If mitochondrial DNA with a harmful mutation becomes the predominant type in a particular tissue, serious symptoms will emerge.
In our JTM paper, work that was primarily supported by the Chronic Fatigue Initiative, we sequenced the mitochondrial DNA from a cohort of ME/CFS patients and healthy individuals, using DNA extracted from white blood cells stored in the biobank developed by the Chronic Fatigue Initiative.
We asked four primary questions:
- Were any of the ME/CFS patients identified by 6 well-known ME/CFS experts misdiagnosed and are actually victims of a mitochondrial genetic disease?
- Do people with ME/CFS carry more copies of mitochondrial DNA with harmful mutations than healthy people (heteroplasmy)?
- Are people belonging to one haplogroup more likely to fall victim to ME/CFS than another?
- Are people who have particular SNPs more likely to experience particular symptoms or have increased severity of symptoms?
Furthermore, we found no difference in the degree of heteroplasmy between patients and healthy individuals.
We also observed no increased susceptibility to ME/CFS among individuals carrying particular haplogroups or SNPs within a haplogroup.
However, we did detect associations of particular SNPs with certain symptoms and/or their severity. For example, we did find that individuals with particular SNPs were more likely to have gastrointestinal distress, chemical or light sensitivity, disrupted sleep, or flu-like symptoms. This finding does NOT mean that if your mitochondrial DNA carries one of these SNPs, you will inevitably experience a particular symptom or have higher severity of some symptoms. Instead, because a particular SNP was seen more often in ME/CFS patients with certain characteristics, individuals that carry that SNP are predicted to be at greater risk of experiencing particular types of symptoms once they become ill.
This study demonstrates the importance of a well-characterized cohort of patients and controls along with detailed clinical information about their experience of illness. Without the data from the lengthy patient questionnaires collected along with the subject’s blood, we could not have correlated SNPs with patient characteristics. While the materials from the CFI subjects are extremely valuable and our results are statistically significant, greater numbers of subjects must be analyzed to determine whether the correlations we detected continue to hold up when more patients are studied, and whether such correlations exist within people carrying other haplogroups.
Due to the European origin of most of the ancestors of the CFI subjects, most belong to haplogroup H, the most common European haplogroup. A much larger number of haplogroup H subjects, as well as large cohorts of individuals with other haplogroups, will be necessary to analyze to dissect out other possible correlations or to determine whether or not any of the correlations we detected with a relatively small population are spurious. With more subjects, we might also be able to detect additional correlations that were not obvious from our initial study.
Whether or not the genetic correlations we have observed are verified or not through further work, our study indicates an important hypothesis that should be tested in ME/CFS. How much of the variation in symptoms between different individuals results from their different nuclear and/or mitochondrial genetic makeup, rather than variation in the inciting cause?
A puzzling aspect of ME/CFS has been the diversity of symptoms and the variation of their severity among different individuals. These differences should not be taken as proof that more than one insult was the initiating factor, nor that different patients have different underlying problems. It remains possible that much of the diversity of the manifestation of the illness results from genetic diversity rather than the existence of multiple fundamental causes.
This article was written by Professor Maureen Hanson and is licensed under a Creative Commons Attribution 4.0 International License.
Maureen R. Hanson
Liberty Hyde Bailey Professor
[email protected]
Phone: 607-254-4833
Fax: 607-255-6249
Hanson Laboratory
Department of Molecular Biology and Genetics
321 Biotechnology Building
Cornell University
Ithaca, NY 14853
Phone: 607-254-4832
 RSS Feed
RSS Feed
